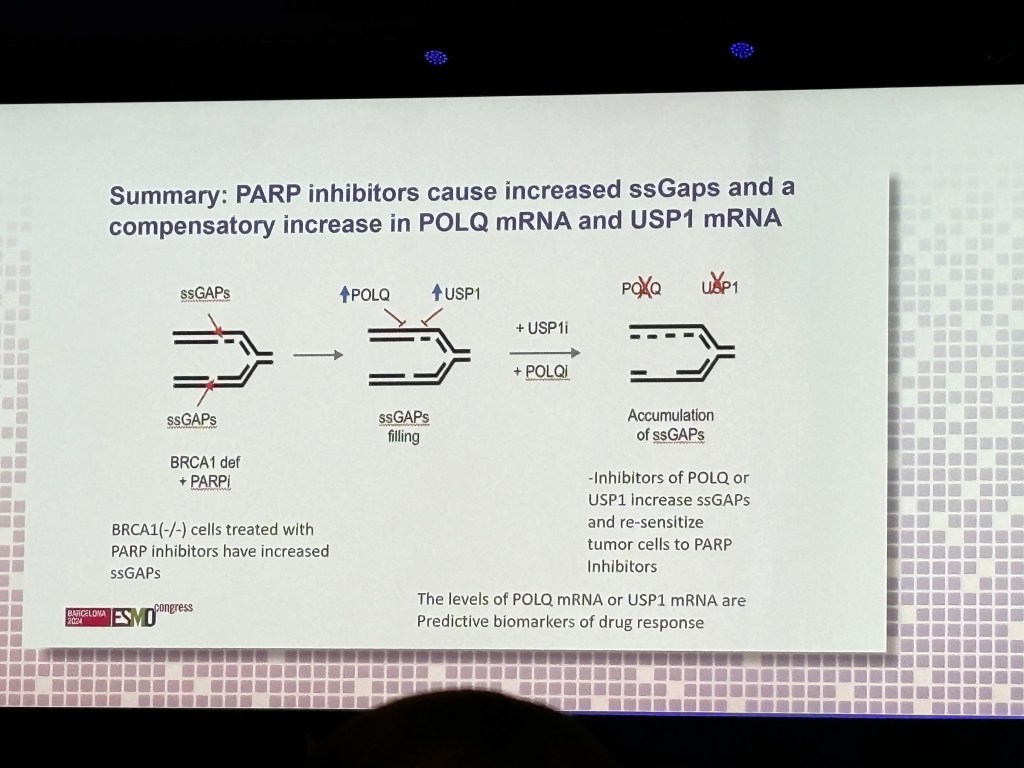
Olaparib and similar drugs have revolutionised the treatment of a sub-set of patients with BRCA gene mutations ( eg Ovarian, Prostate, Breast cancers).
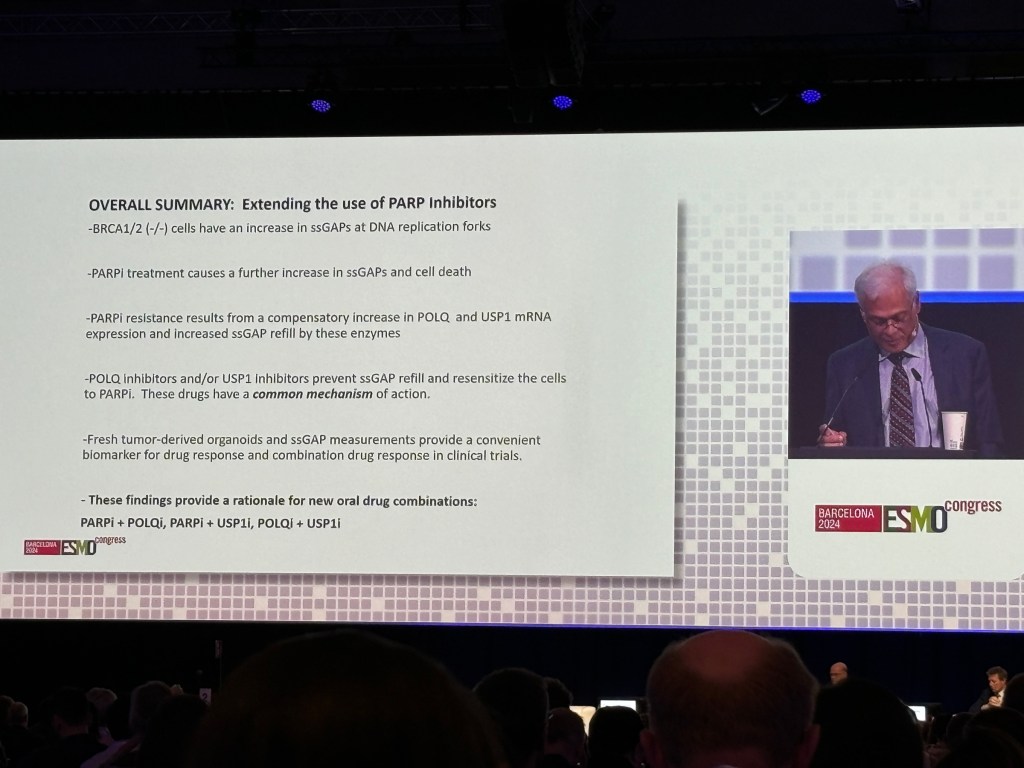
But patients can develop resistance to these drugs.
At the ESMO European Society of Medical Oncology Congress-2024, Barcelona), ways to overcome this resistance was discussed.
Targeting the Enzymes USP-1 and POLQ seems to overcome resistance.
The future looks promising!
Disclaimer: Please note – This blog is NOT medical advice. This blog is NOT a expert medical opinion on various topics. This blog is purely for information only and do check the sources where cited. Please DO consult your own doctor to discuss concerns and options relevant to you. The views expressed in this blog are NOT, in any way whatsoever, intended to be a substitute for professional advice. The blog is NOT previewed, commissioned or otherwise endorsed, in any way, by any organisation that the author is associated with. The views expressed in this blog likely represents some of the author’s personal views held at the time of drafting the blog and MAY CHANGE overtime, particularly when new evidence comes to light.
At the recent ESMO congress, new data was presented showing that upfront treatment with Abiraterone helps patients liver longer.
Hormone injections plus Chemotherapy is standard of care for new diagnosed advanced prostate cancer ( doublet treatment).
A French trial ( PEACE 1) explored the use of Abiraterone in this setting. The investigators found that a “triplet treatment” of Abiraterone + Chemotherapy + Hormone injections would make people live substantially.
This is likely to become standard of care in near future.
Another U.K. trial ( STAMPEDE) assessed Abiraterone in the High risk but less advanced prostate cancer. The study found that adding Abiraterone to the other treatments can improve survival of prostate patients.
Disclaimer: Please note – This blog is NOT medical advice. This blog is NOT a expert medical opinion on various topics. This blog is purely for information only and do check the sources where cited. Please DO consult your own doctor to discuss concerns and options relevant to you. The views expressed in this blog are NOT, in way whatsoever, intended to be a substitute for professional advice. The blog is NOT previewed, commissioned or otherwise endorsed, in any way, by any organisation that the author is associated with. The views expressed in this blog likely represents some of the author’s personal views held at the time of drafting the blog and MAY CHANGE overtime, particularly when new evidence comes to light.
The Staff at National Health Service in UK are doing an admirable job during the pandemic. In the particular, the frontline staff (“patient-facing”) are showing great courage in face of great difficulties and are primarily driven by altruism.
But the pressures of pandemic means many routine scans and hospital clinic appointments have been cancelled particularly during the first wave. There is a great worry about delayed diagnosis of cancer and delayed treatment of cancer.
A paper in BMJ reports that cancer patients survival can be significantly compromised.
But, as with everything else in life, things are not always what they look like at first impression. Even things that are logical and common sense at first glance do not turn out to be simple and clear.
Firstly, delays and cancellations of scans paradoxically could have psychologically benefited some cancer patients . This might seem counterintuitive or even an outrageous statement.
But there are some cancers which are being over diagnosed. A Cancer diagnosis does not always mean a death sentence. Some cancers do not cause problems for a long time or never in the life time of a person. These cancers do not need to be diagnosed promptly. Not being diagnosed with these cancers prevents the psychological burden of a cancer diagnosis. This “over diagnosis” would be expectedly less during pandemic.
Secondly, treatment delays could be caused by a cancer that is advanced and the need for time consuming additional investigations and procedures. Sometimes delays are caused by patients needing to see many medical specialists for the treatment. So it’s the aggressive cancer and the complex patient care that would cause the delay and is responsible for poor outcome rather than the delay by itself.
The old adage “prevention is better than cure” is mostly true with regards to cancer if you can do it.
If you can’t prevent it , at least catch it early, has been the prime motive behind screening tests for breast, cervical, bowel, lung and prostate cancers. (“early is better”). Cancers that are detected at an early stage can offer a better chance of curative treatment.
So one might logically expect that intensive monitoring and early diagnosis of a cancer relapse or a secondary cancer after initial treatment can be immensely helpful.
But the evidence for intensive hospital follow-up visits and investigations is weak for most cancers except for some cancers such as Testicular Cancers which are highly curable.
Intensive monitoring after bowel cancer treatment can detect treatable cancers. To confirm the benefit of early detection of relapse by intensive monitoring , a trial was conducted comparing intensive follow up versus routine follow up ( in France and Belgium).
Data presented at ESMO ( European Society of Medical Oncology) shows that the intensive follow with scans can detect cancer recurrences which can be treated by further surgery. But unfortunately the intensive follow up did NOT lead to longer life expectancy.
The results might be counterintuitive but after an average follow up more than six years, this trial demonstrates that intensive follow is NOT always best. Scans might be done for psychological reassurance but they could end up causing significant anxiety.
When there are resource constraints (e.g low economic countries) , one has to be careful about frequents routine scans for those without symptoms.
During COVID-19, even in rich countries such as UK where there might be huge waiting lists, one has to consider prioritising scans for those who need most.
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only and do check the the sources where cited. Please consult your own doctor to discuss concerns and options relevant to you.
The views expressed in this blog represent the author’s views held at the time of drafting the blog and is likely to change overtime, particularly when new evidence comes to light. The blog is not necessarily endorsed by any organisation the author is associated with and views are not substitute for professional advice.
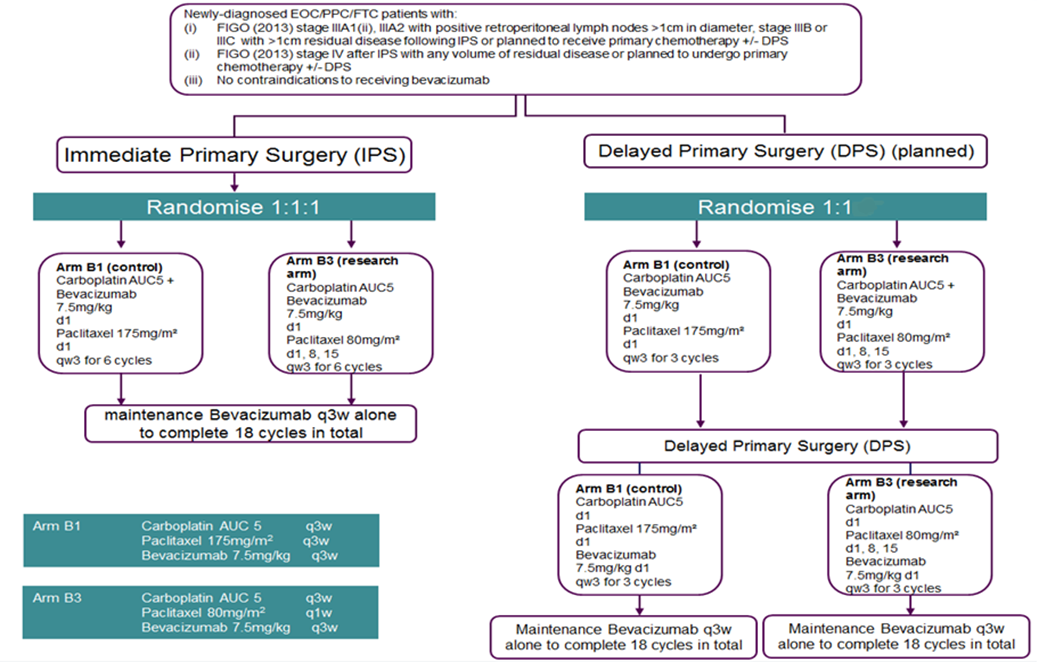
Advanced ovarian cancer is treated by chemotherapy. A pre ious study of Japanese ovarian cancer patients RT showed significantly increased survival in those treated with dose-dense weekly paclitaxel compared to the standard three-weekly schedule.
Data from an international trial called ICON8 was presented at the ESMO Virtual Congress 2020, this week.
The final analysis of ICON8 “provides conclusive evidence that although weekly dose-dense chemotherapy can be successfully administered as first-line treatment for ovarian cancer, it has no survival advantage over the standard chemotherapy given once every 3 weeks.
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only and do check the the sources where cited. Please consult your own doctor to discuss concerns and options relevant to you.
The views expressed in this blog represent the author’s views held at the time of drafting the blog and is likely to change overtime, particularly when new evidence comes to light. The blog is not necessarily endorsed by any organisation the author is associated with and views are not substitute for professional advice.
References 1. Dexamethasone and supportive care with or without whole brain radiotherapy in treating patients with non-small cell lung cancer with brain metastases unsuitable for resection or stereotactic radiotherapy (QUARTZ): results from a phase 3, non-inferiority, randomised trial. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(16)30825-X/fulltext
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only and do check the the sources where cited. Please consult your own doctor to discuss concerns and options relevant to you.
The views expressed in this blog represent the author’s views held at the time of drafting the blog and is likely to change overtime, particularly when new evidence comes to light. The blog is not necessarily endorsed by any organisation the author is associated with and views are not substitute for professional advice.
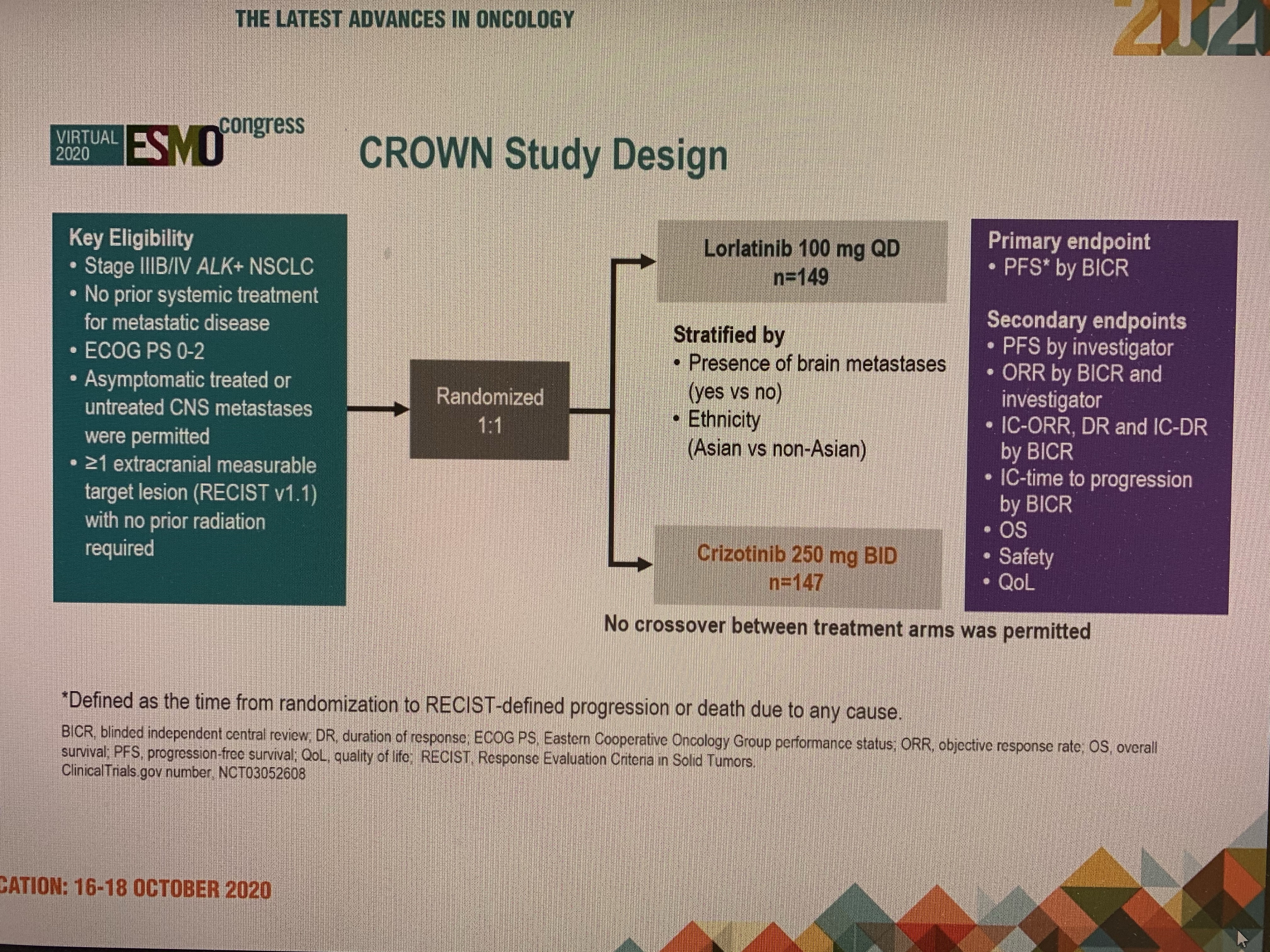
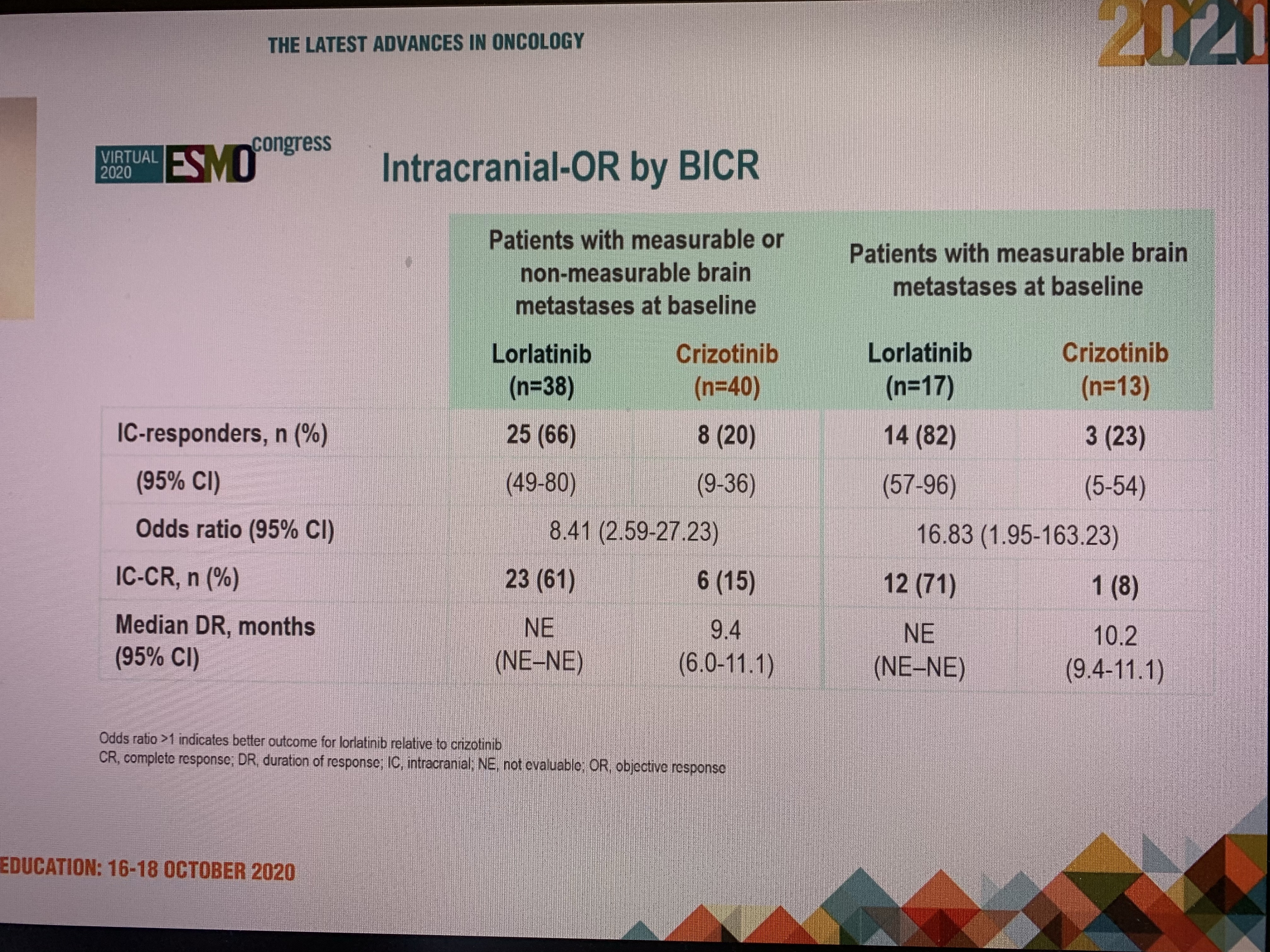
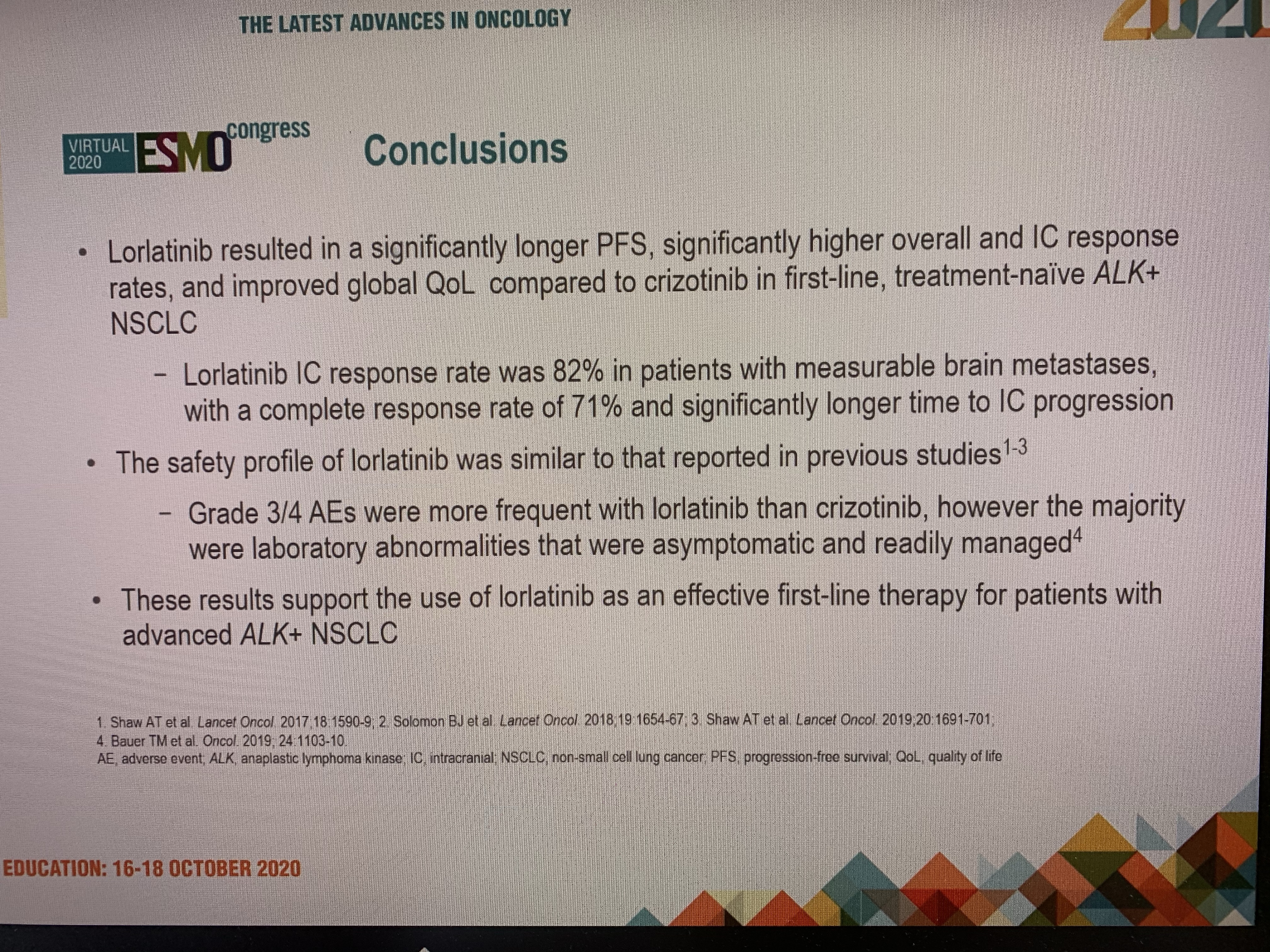
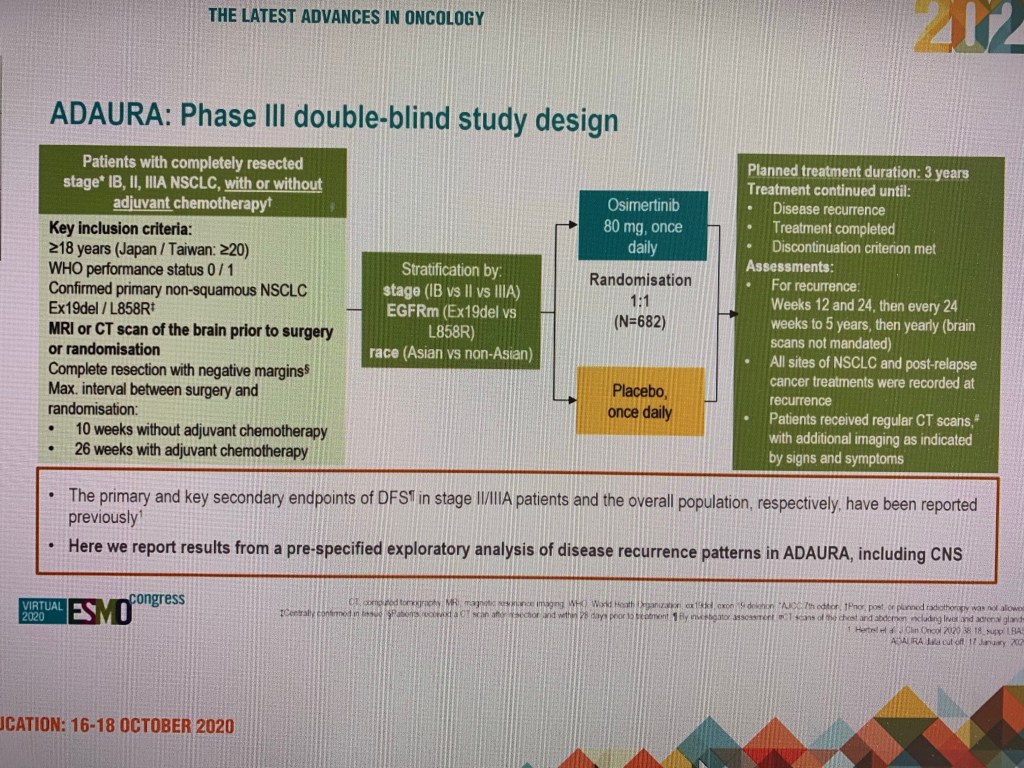
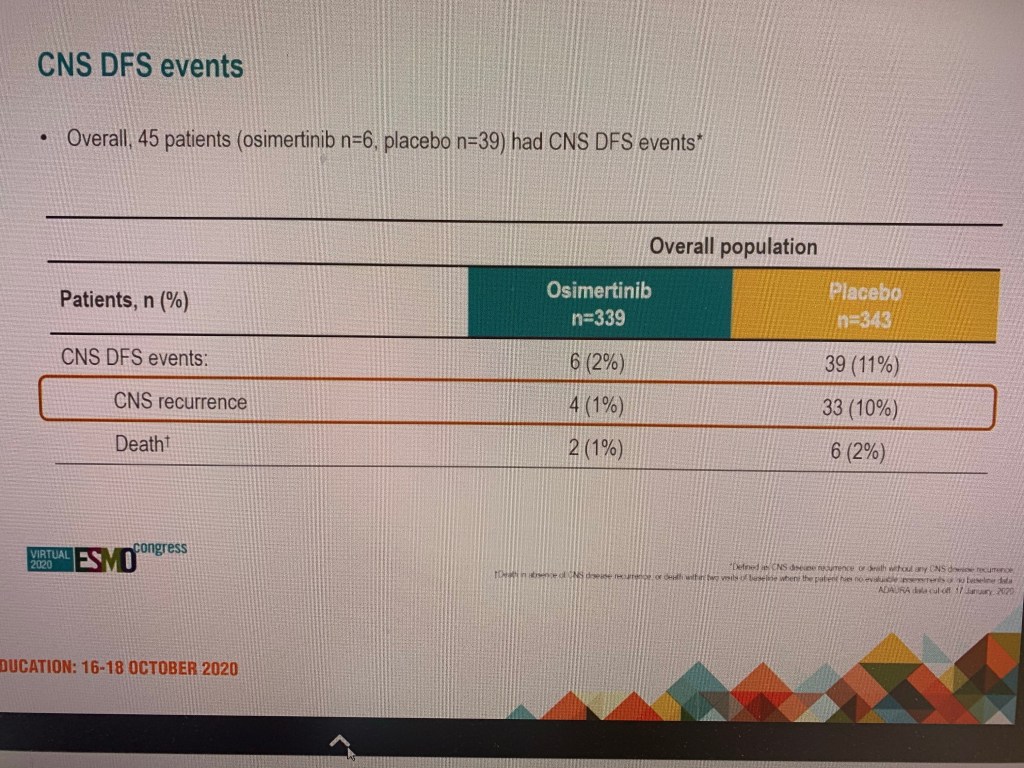
Traditional intravenous Chemotherapy agents are often thought NOT to be highly effective in treating and preventing brain secondaries. This is because of the penal blood brain barrier.
Data presented at ESMO ( European Society of Medical Oncology) presidential symposium shows that the Osimertinib is highly active and significantly reduces risk of brain secondaries.
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only and do check the the sources where cited. Please consult your own doctor to discuss concerns and options relevant to you.
The views expressed in this blog represent the author’s views held at the time of drafting the blog and is likely to change overtime, particularly when new evidence comes to light. The blog is not necessarily endorsed by any organisation the author is associated with and views are not substitute for professional advice.
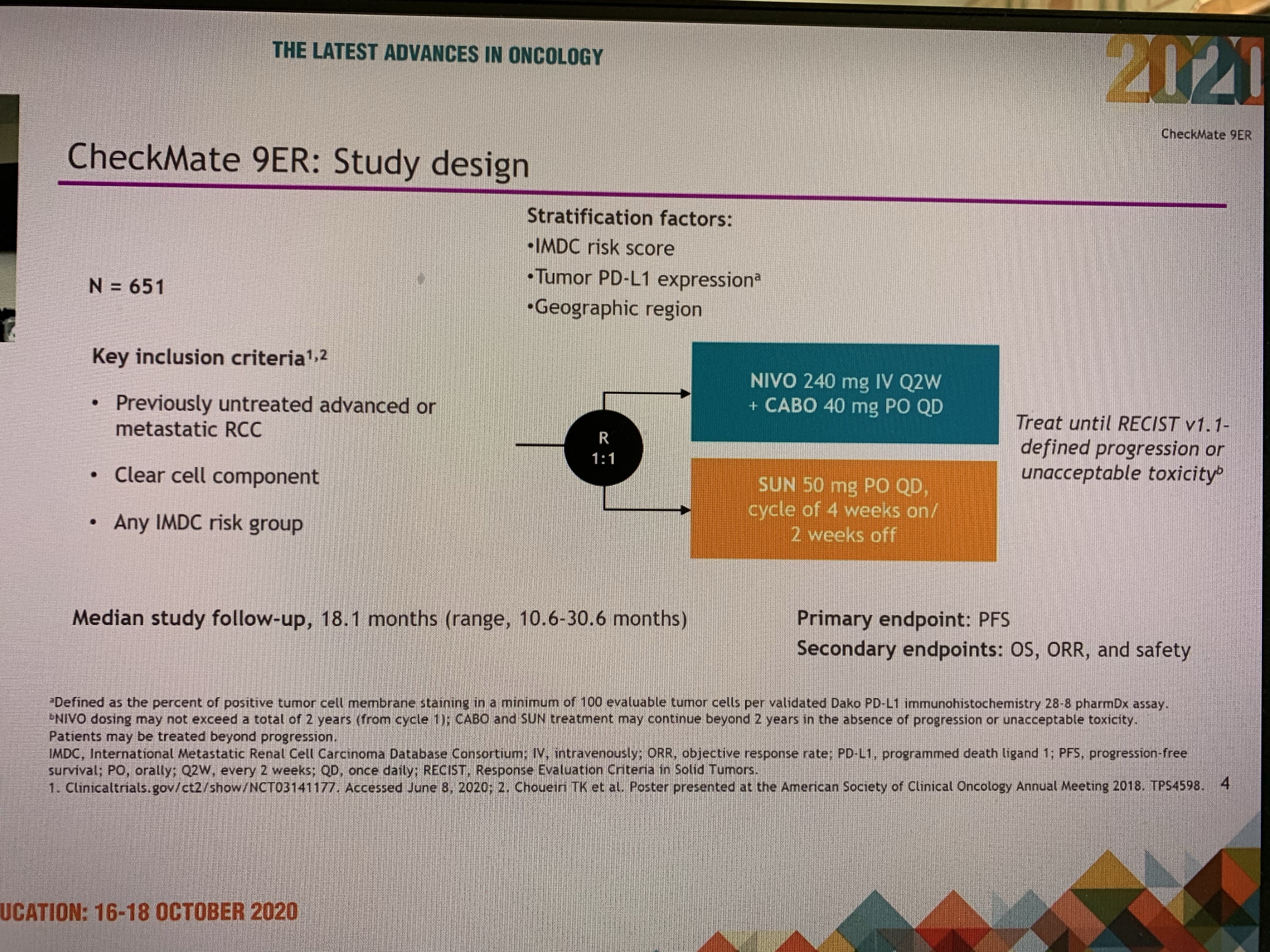
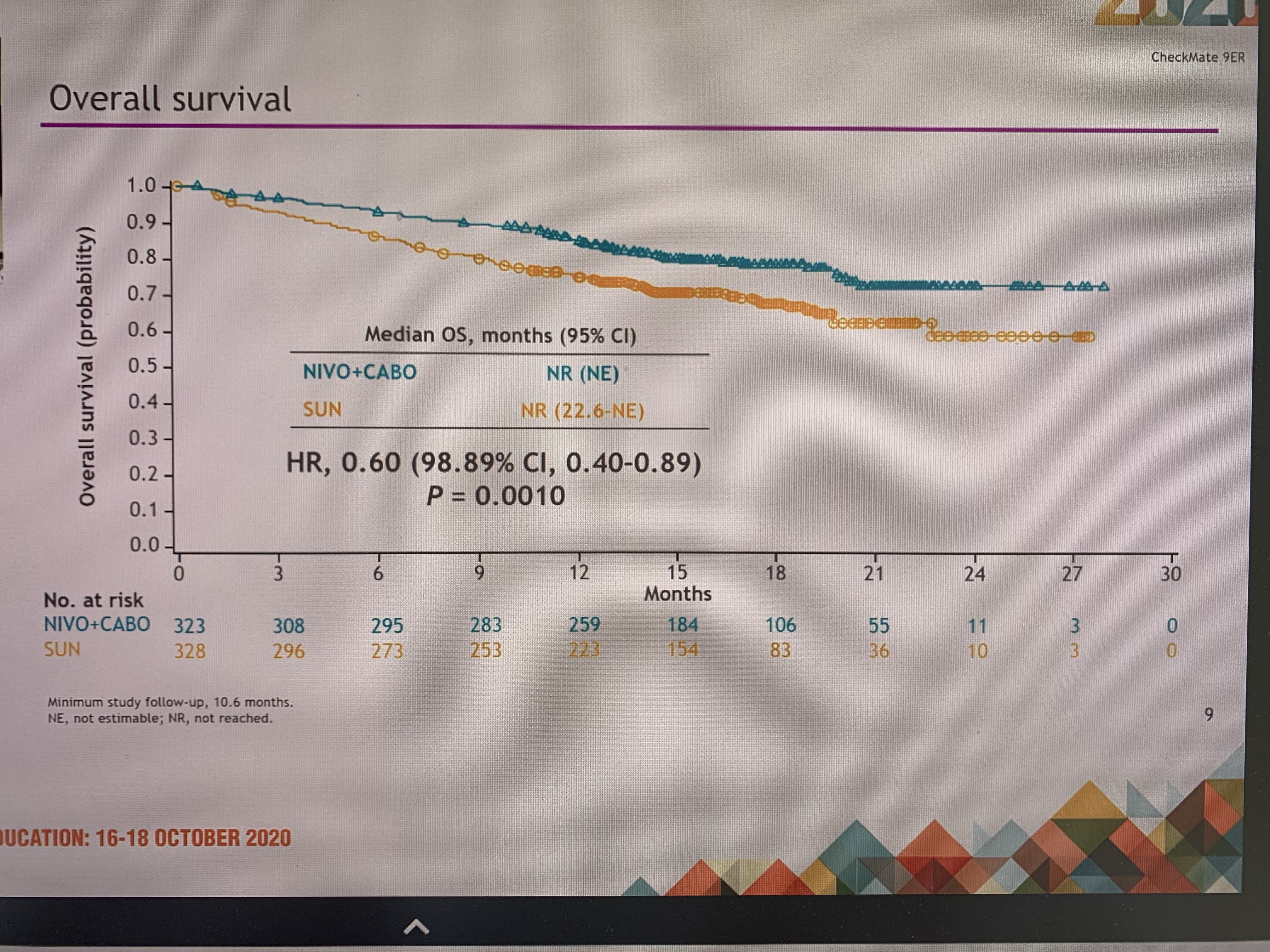
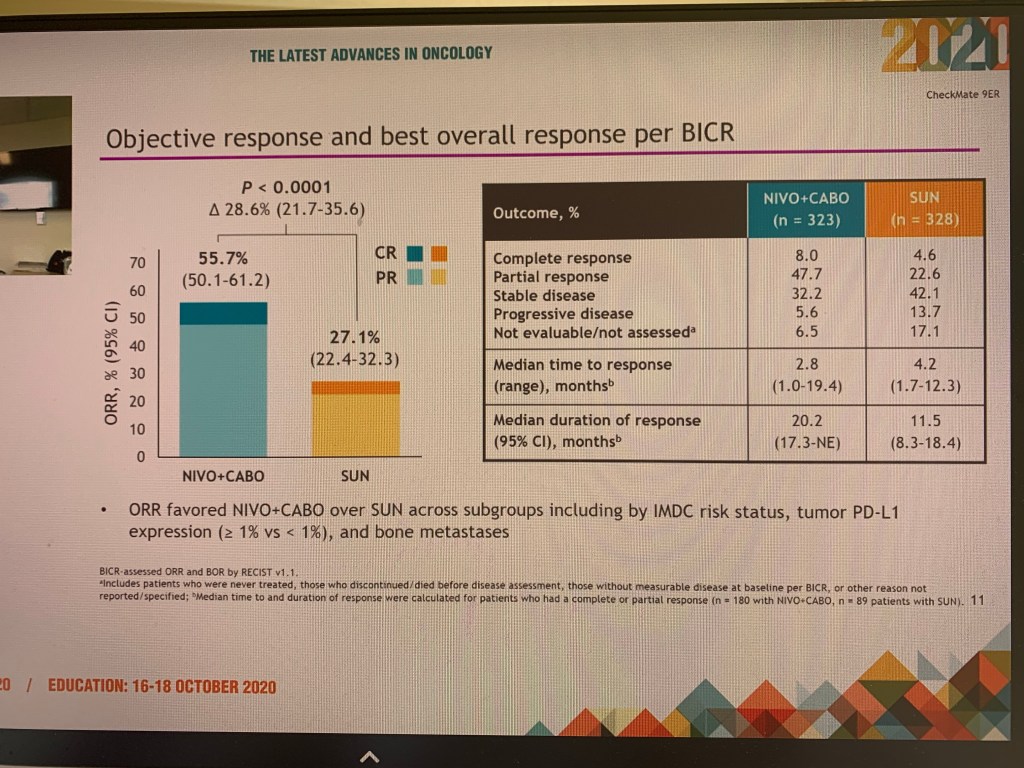
The treatment of kidney cancer has dramatically changed in the last decade. More treatments are in pipeline and there was more exciting news this week.
Upfront immunotherapy in combination with other agents is very promising in 1st line treatment of advanced kidney cancers.
“Nivolumab and Cabozantinib” combo joins the other combos “Nivolumab and Ipililumab” and “Pembrolizumab and Axitinib “ as 1st line options
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only and do check the the sources where cited. Please consult your own doctor to discuss concerns and options relevant to you.
The views expressed in this blog represent the author’s views held at the time of drafting the blog and is likely to change overtime, particularly when new evidence comes to light. The blog is not necessarily endorsed by any organisation the author is associated with and views are not substitute for professional advice.
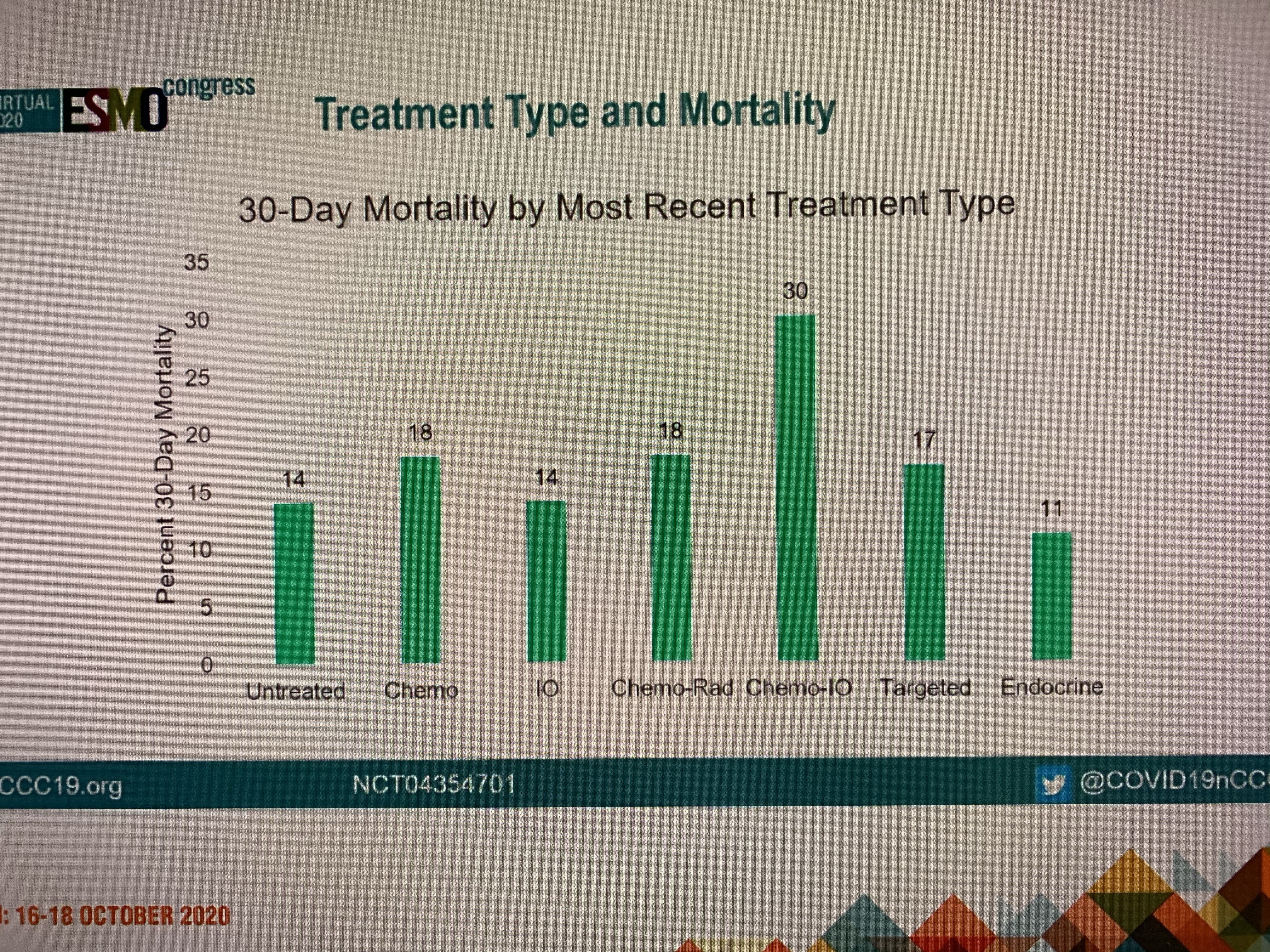
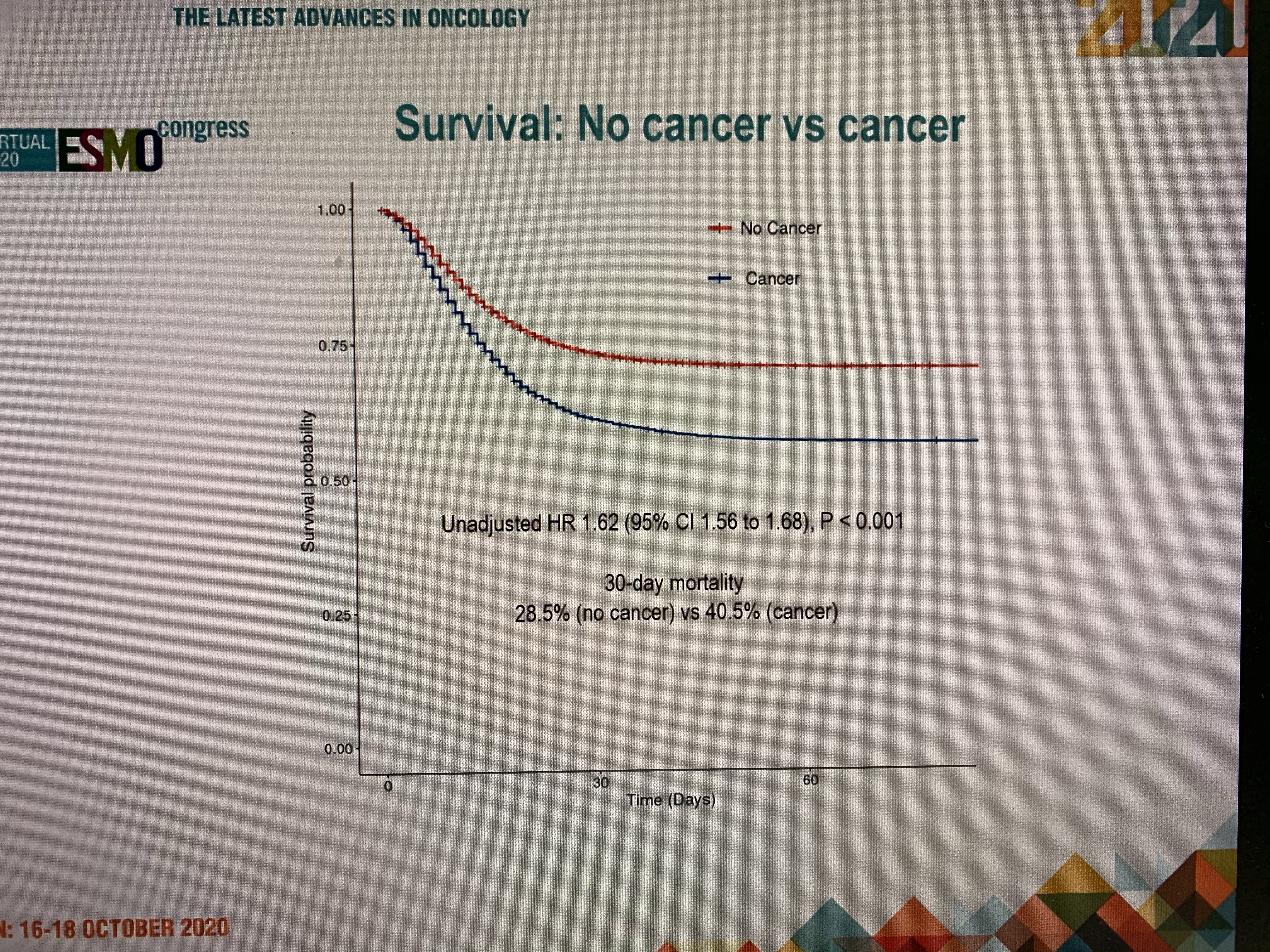
Elderly cancer patients on the whole did very badly but surprisingly cancer patients under age of 50 did far worse than their peers without cancer.
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only and do check the the sources where cited. Please consult your own doctor to discuss concerns and options relevant to you.
The views expressed in this blog represent the author’s views held at the time of drafting the blog and is likely to change overtime, particularly when new evidence comes to light. The blog is not necessarily endorsed by any organisation the author is associated with and views are not substitute for professional advice.
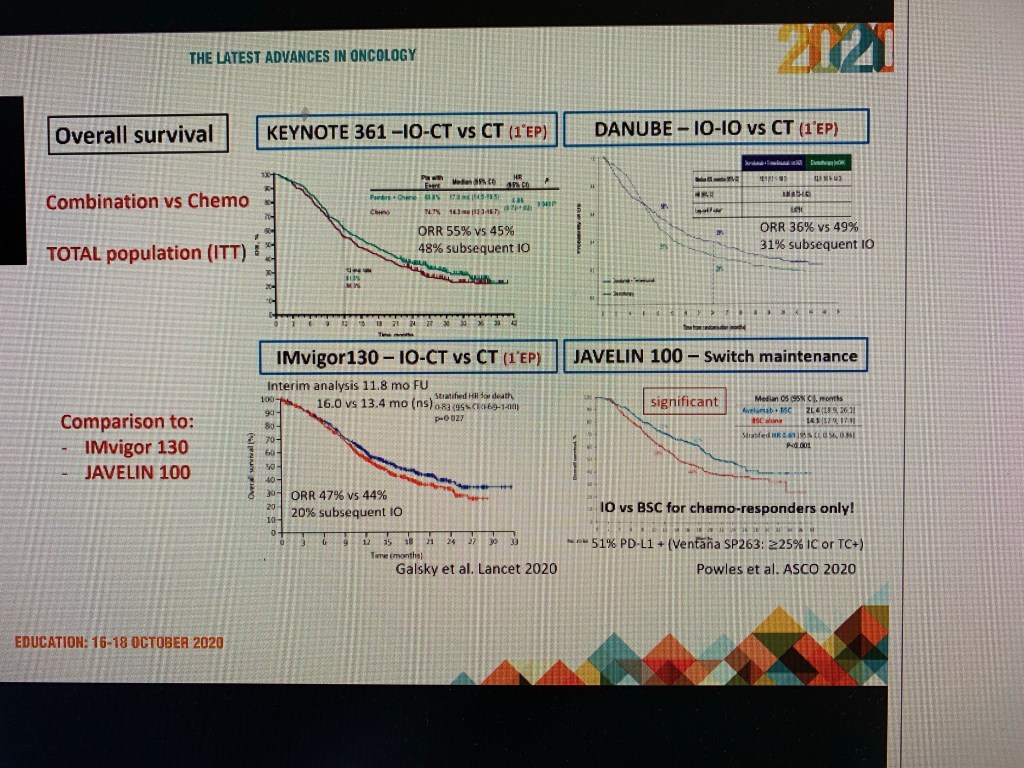
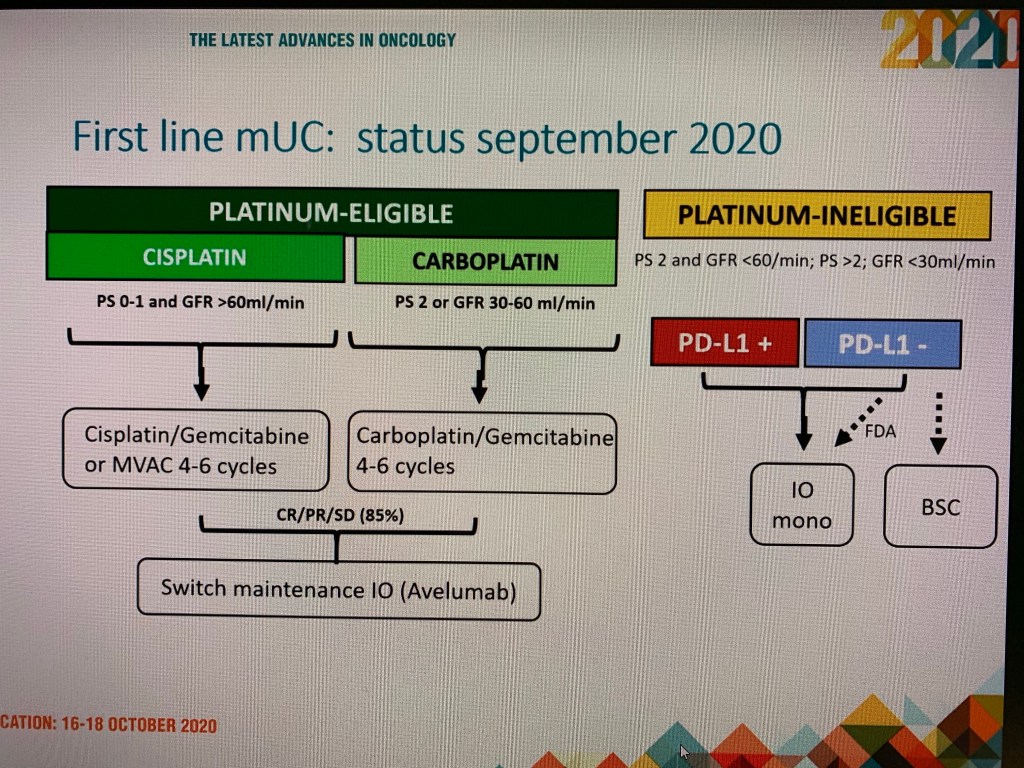
Immunotherapy has revolutionised the treatment of many advanced cancers such Skin cancer Melanoma and Kidney cancers.
Immunotherapy is a standard treatment for 2nd line treatment of bladder cancer.
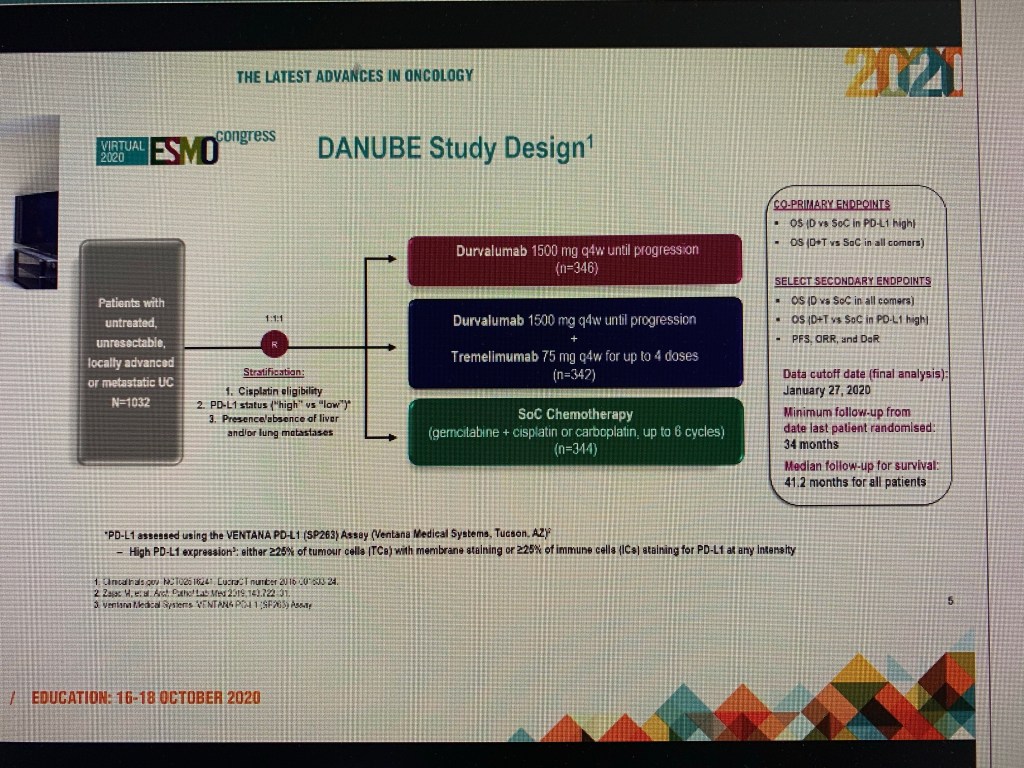
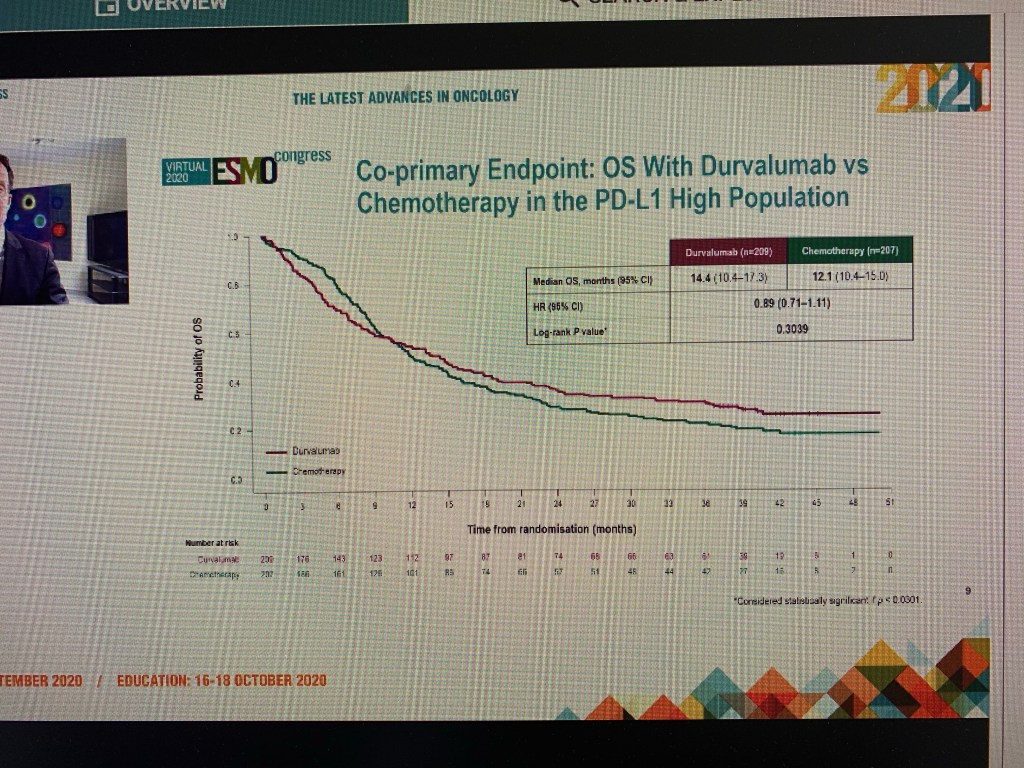
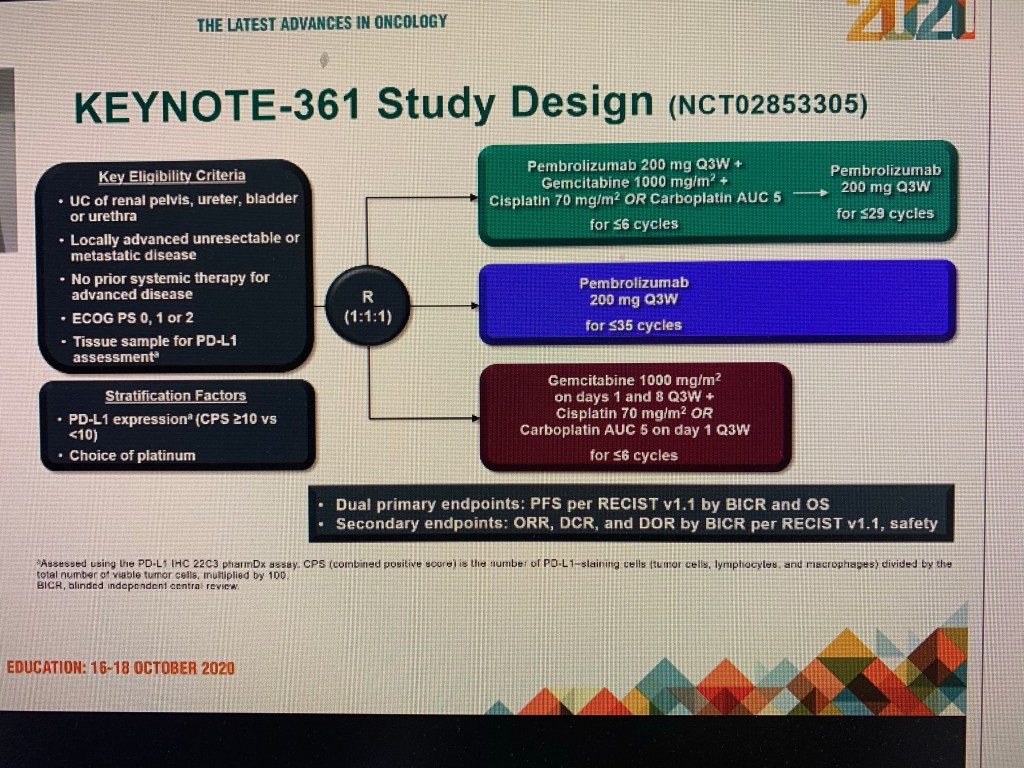
Two recent trials presented at ESMO virtual meeting explored the use of immunotherapy in 1st line setting. (Pembrolizumab and Durvalumab).
Immunotherapy alone, or in combination with Chemotherapy was not superior even in patients selected by markers thought to favour immunotherapy alone.
For most bladder cancer patients immunotherapy remains a excellent 2nd line option or as a maintenance treatment option.
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only and do check the the sources where cited. Please consult your own doctor to discuss concerns and options relevant to you. The views expressed in this blog represent the author’s views held at the time of drafting the blog and is likely to change overtime, particularly when new evidence comes to light. The blog is not necessarily endorsed by any organisation the author is associated with and views are not substitute for professional advice.
The hormone injections reduce the Testosterone in men.
Now a new medication, called Relugolix, has been successfully tested in clinical trials. Relugolix, unlike other first line hormone injections , can be taken by mouth instead.
Relugolix also has the advantage of not only working rapidly but also has the advantage of stopping to work quickly when it is withdrawn. This is unlike the injections which take a while to work but also do not stop working quickly when injections are stopped.
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only and do check the the sources where cited. Please consult your own doctor to discuss concerns and options relevant to you.
The views expressed in this blog represent the author’s views held at the time of publication and is likely to change overtime, particularly when new evidence comes to light. The blog is not necessarily endorsed by any organisation the author is associated with and views are not substitute for professional advice.
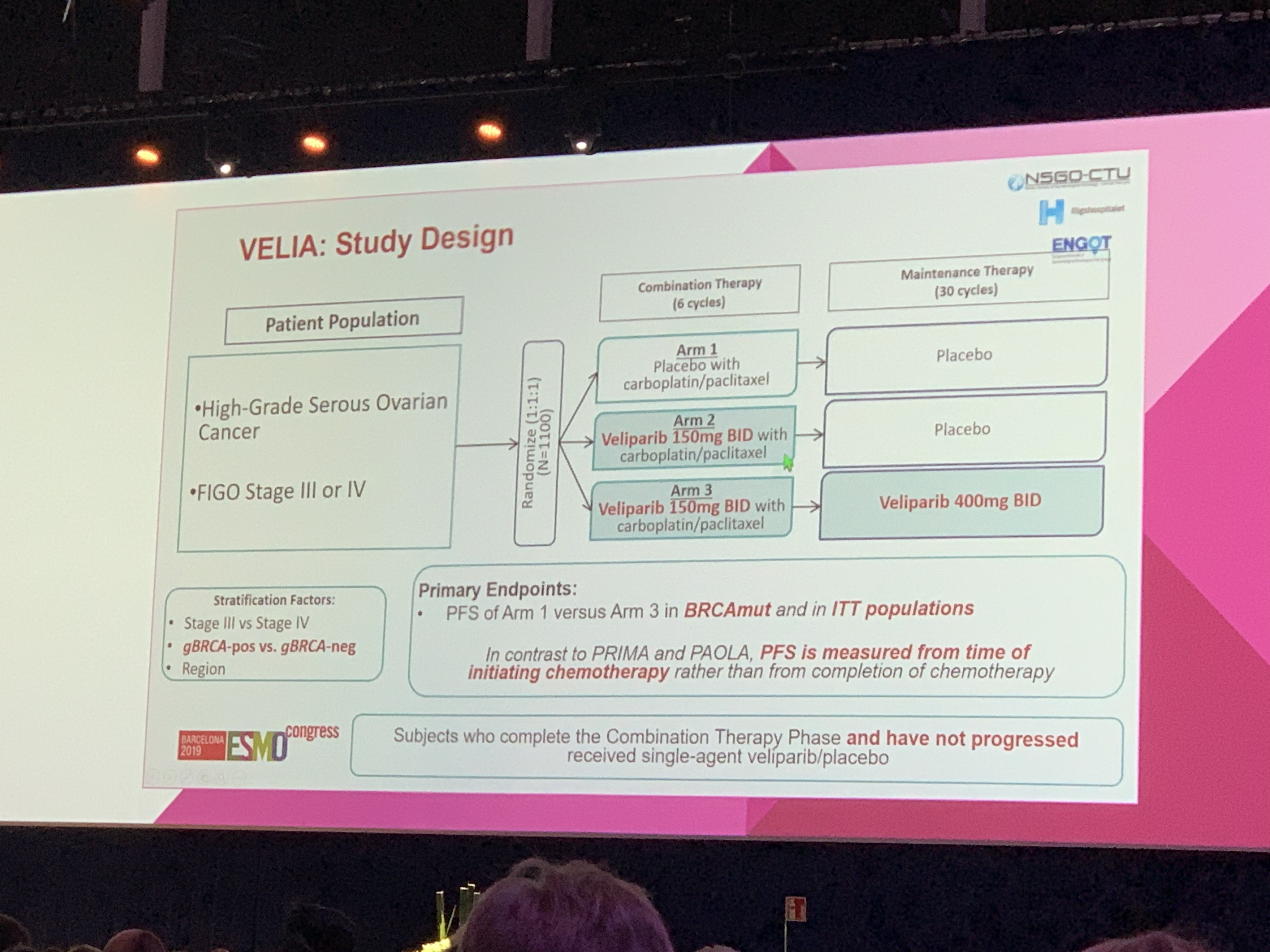
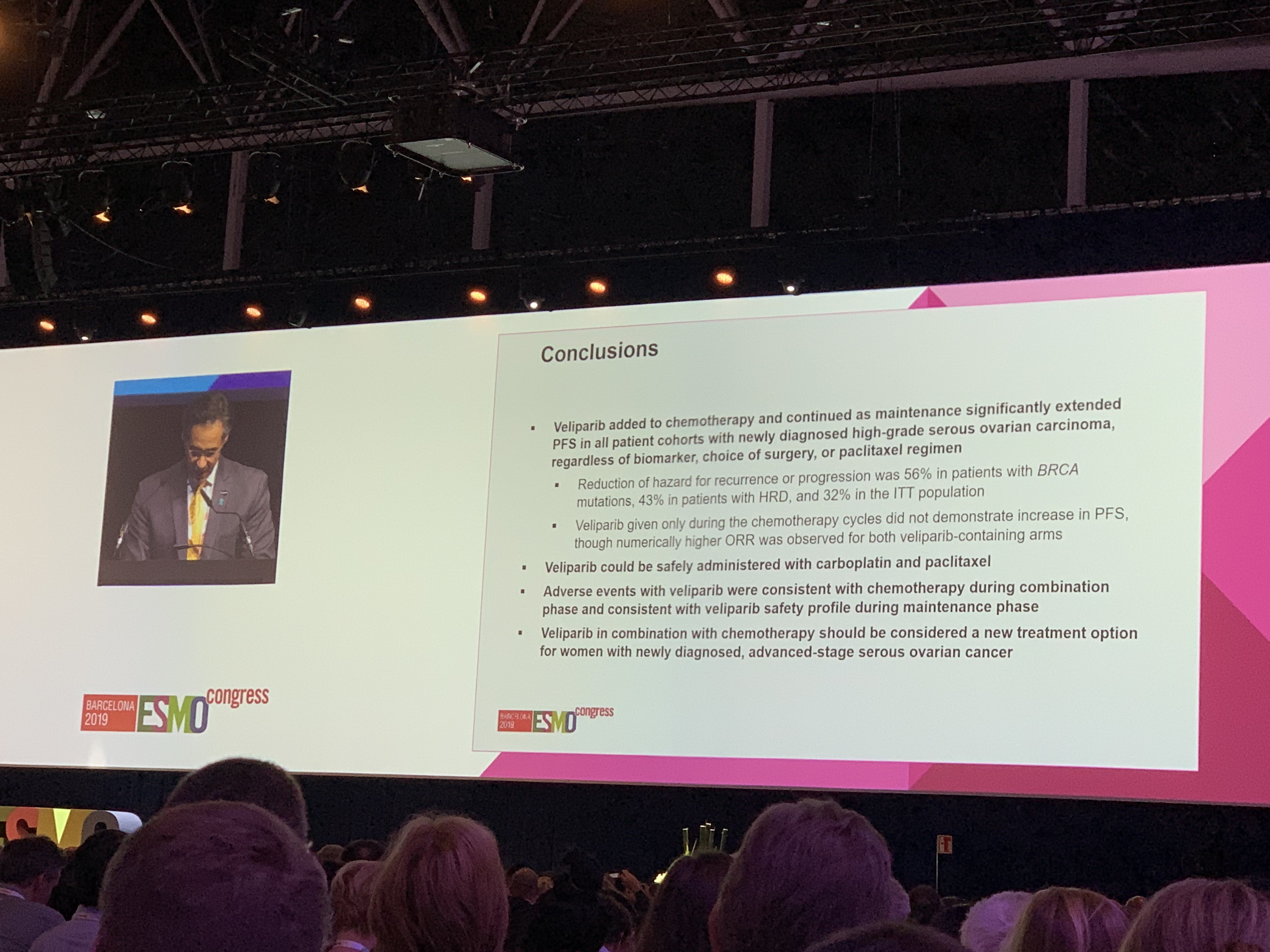
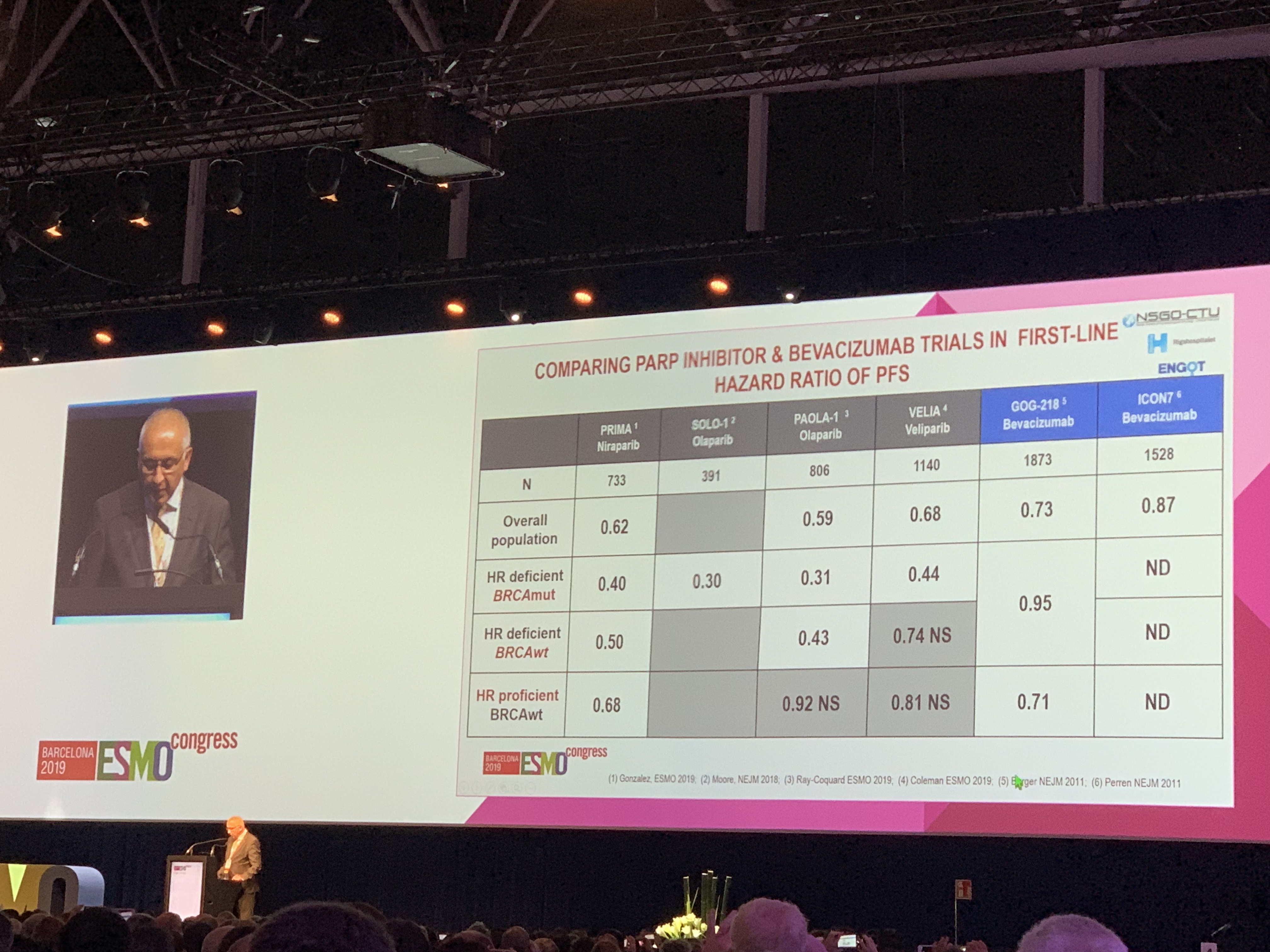
Veliparib trial data has certainly brought more options to the table in treatment of advanced Ovarian cancer.
Trial data presented at ESMO congress at Barcelona shows that first line therapy with Veliparib is beneficial.
Acknowledgement: Copyright of Slides: Authors and ESMO
References
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only. See your own doctor to discuss concerns and options relevant for you.
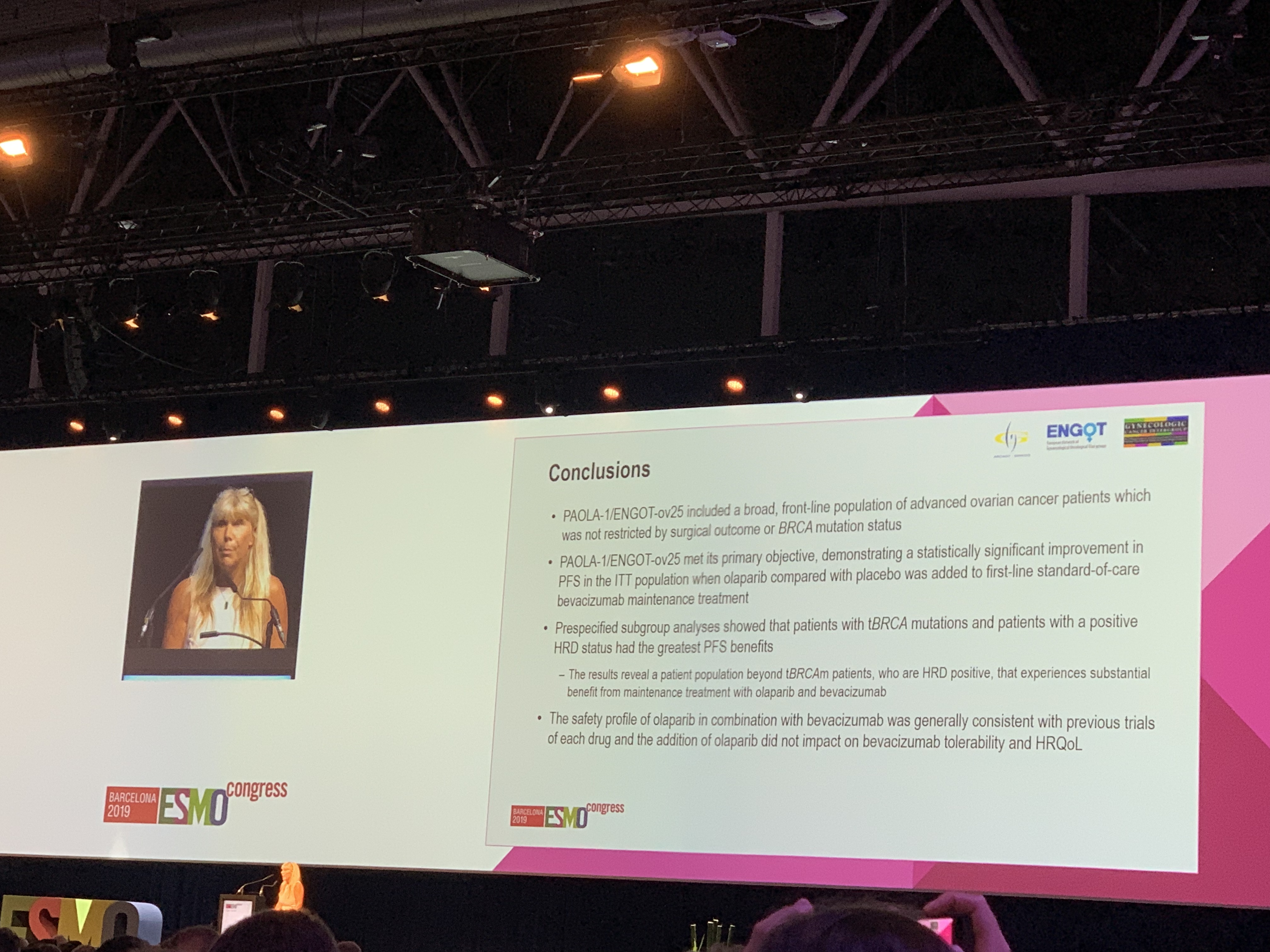
New trial data presented at the ESMO cancer Congress 2019 in Barcelona, Spain, show excellent results for the combination of Olaparib and Bevacizumab. The combination looks likely to become standard of care in at-least a subgroup of patients.
The expert discussing the trial data did raise the possibility that most benefit seems to come from Olaparib in patients with BRCA mutations and whether Olaparib alone instead combination is enough for this group. More data is awaited.
References
1. ESMO 2019 congress press release. Ovarian Cancer: More Women Benefit from Maintenance Combined Targeted Therapy [ESMO 2019 Press Release]
Acknowledgement: Copyright of Slides: Authors and ESMO
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only. See your own doctor to discuss concerns and options relevant for you.
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only. See your own doctor to discuss concerns and options relevant for you.
This is because patients in this study were followed up only for about 2 years ( to be precise a median follow up of only 26 months) . More long term follow up is needed before firm conclusions could be drawn.
Disclaimer: Please note- This blog is NOT medical advice. This blog is purely for information only. See your own doctor to discuss concerns and options relevant for you.