
Advanced Gall bladders and bile duct cancers are difficult to control for long periods.
Some of these Gall bladder cancers carry an abnormality called “FGFR2 rearrangement” .
These changes can be targeted by a drug called Pemigatinib and at present, it is only used in 2nd line setting.
A recent trial evaluated this ORAL drug in 1st line setting and compared this drug with the standard INTRAVENOUS chemotherapy.
The study results were presented and discussed at the ASCO 2026 Annual Meeting in Chicago ( ASCO- American Society of Clinical Oncology).
Pemigatinib in 1st line setting showed an impressive response rate of 47% compared 15% response rate with chemotherapy.
The median duration of response was 14.2 months for Pemigatinib versus 6.3 months in chemotherapy arm.
Somewhat disappointingly the better response rates did not to longer survival for Pemigatinib. Median OS was similar (24.4 versus 25.0 months, respectively). This might be partly because of cross over patients from chemotherapy arm to the trial arm.
Nevertheless, this ORAL therapy is a good alternative option for patients who are not suitable for platinum-based chemotherapy regimens or for those patients who prefer to avoid intravenous chemotherapy.
Another word of caution: only a small minority of Gall bladder cancers are found to contain the molecular change called “FGFR2 rearrangement”.
For instance for this study, the investigators had to prescreen 4563 patients to find 196 potentially suitable patients.
For the minority who have this FGFR2 rearrangement, Pemigatinib is a good option to consider.
References
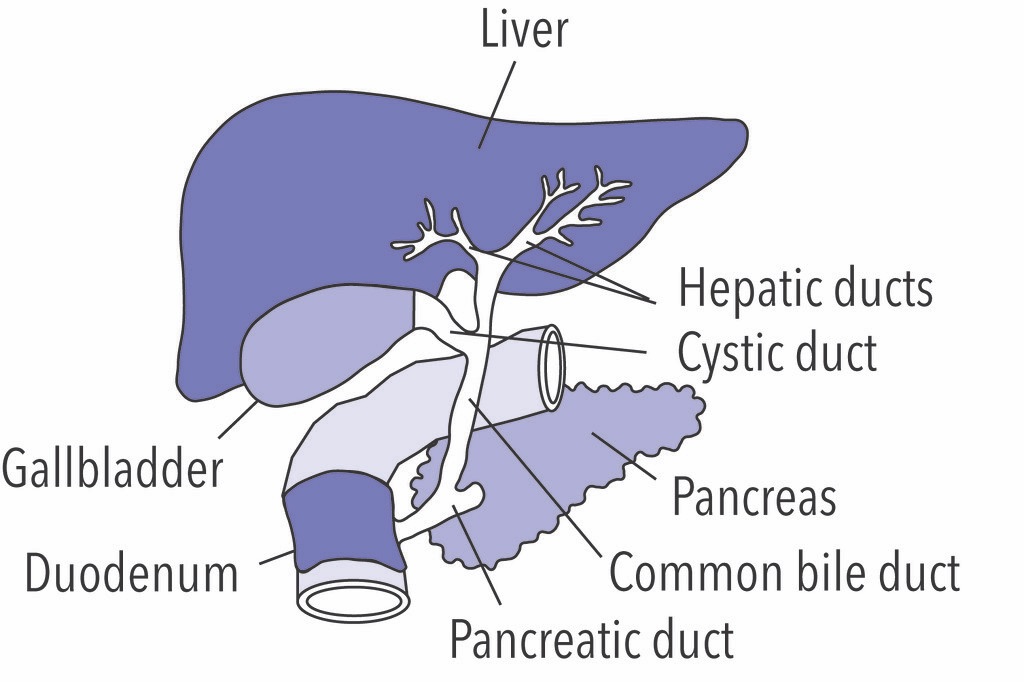
Gallbladder image source: Image source: https://live.staticflickr.com/1696/24312875104_9c297a2d1e_b.jpg
Disclaimer: Please note – This blog is NOT medical advice. This blog is NOT a expert medical opinion on various topics. This blog is purely for information research only and do check the sources where cited. But the author cannot vouch for scientific integrity of the sources cited and author is not responsible for any information in any advert on those cited pages. Please DO consult your own doctor to discuss concerns and options, which are directly relevant and specific to you. The views expressed in this blog are NOT, in any way whatsoever, intended to be a substitute for professional advice. The blog is NOT previewed, commissioned or otherwise endorsed, in any way, by any organisation that the author is associated with. The views expressed in this blog likely represents some of the author’s personal views held at the time of drafting this blog and MAY CHANGE overtime, particularly when new evidence comes to light.

{kind=link}