There is a significant social media promotion of these two drug combination- fenbendazole and ivermectin – for treatment of prostate cancer.
They are relatively cheap and so cost is not a major hindrance.
Are they both any good for routine clinical use ?
The short answer is NO.
Both Ivermectin and Fenbendazole are drugs currently licensed for treatment of human and / or animal infections.
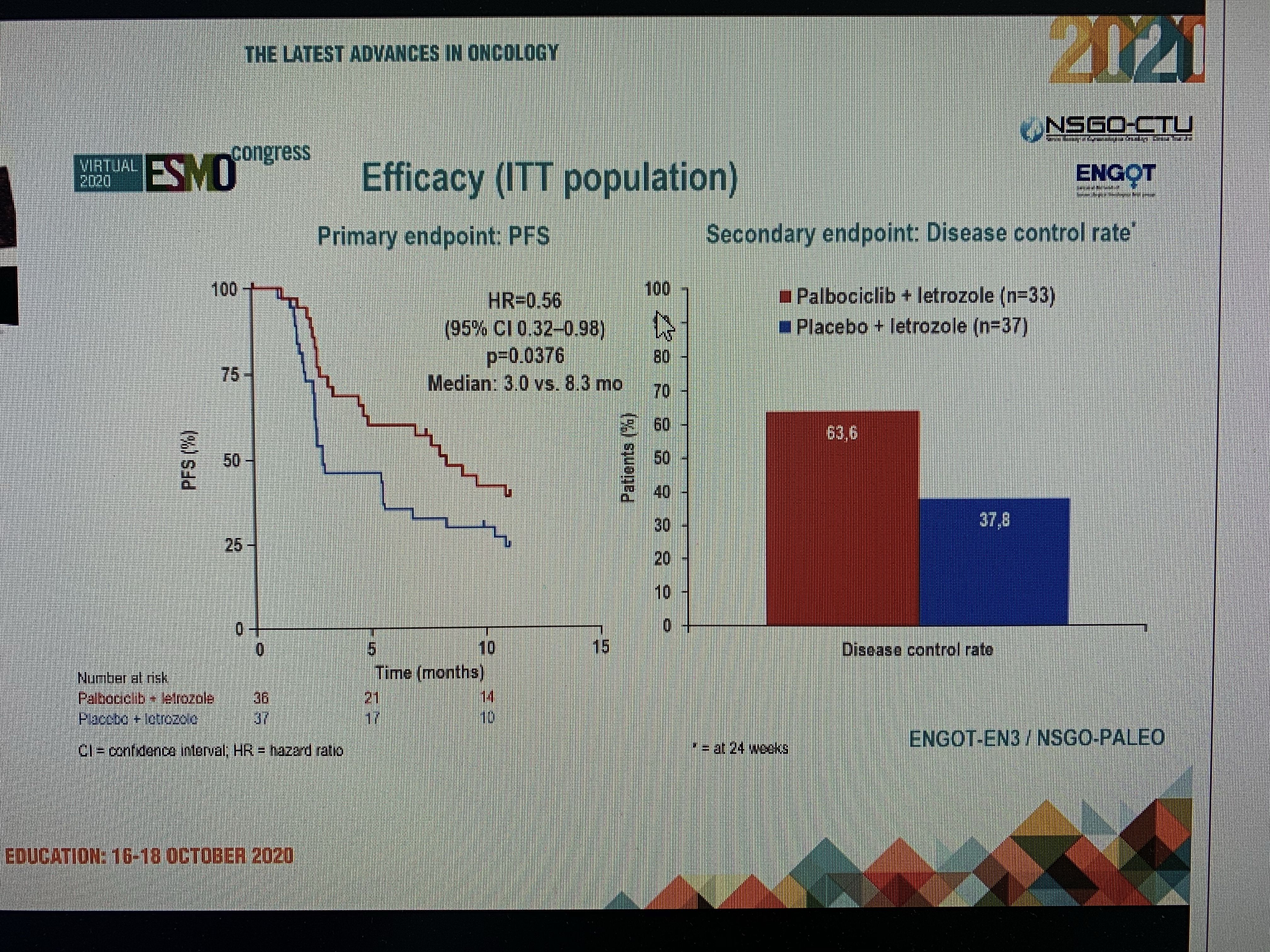
There is lot of pre-clinical laboratory evidence to indicate anti-cancer activity regarding these two drugs. But that does not mean they can be safely used clinically. Good clinical trials are needed before they can be used clinically .
Remember both drugs can have significant side effects. ( Ivermectin . Fenbendazole ).
For instance, these drugs can cause liver damage. They can cause nausea, stomach pain, muscle pain, joint pain and in worse cases cause mental changes.
Advanced cancer patients are desperate to try anything. It’s human nature to fight . But that doesn’t mean trying “unproven treatments” are a good idea. This is because the side effects of the drugs can make cancer patients life even more miserable.
Both the drugs – Ivermectin and Fenbendazole- can also interfere with other cancer treatments.
Scientifically, we cannot 100% rule out that a derivative of Ivermectin or Fenbendazole might be repurposed for cancer treatment in future.
But it is NOT a good idea to use Ivermectin or Fenbendazole as an anti-cancer treatment in routine clinical practice NOW.
Be careful. Discuss your concerns with your doctor.
Be aware of scams.
Also be very careful about friends, family members and well wishers – with good intentions – but unknowingly passing misleading information to you !

References
Macmillan. Cancer and ivermectin: What people with cancer need to know. Richard Simcock Chief Medical Officer and Macmillan. Published: 01 October 2025
Ivermectin European Data sheet. Accessed 1st Feb 2026. Patient information leaflet.
Fenbendazole. DEFRA. VETERINARY MEDICINAL PRODUCT. Accessed 1st Feb 2026.
Ivermectin Review: Ivermectin, a potential anticancer drug derived from an antiparasitic drug
Fenbendazole: Oral Fenbendazole for Cancer Therapy in Humans and Animals. Jolie Nguyen et al. Anticancer Res. 2024 Sep
Ivermectin: Integrated analysis reveals FOXA1 and Ku70/Ku80 as targets of ivermectin in prostate cancer.
False information on ivermectin continues to circulate worldwide. Published on May 14, 2025 at 22:01. Updated on May 16, 2025 at 06:59. By Ede ZABORSZKY.

Disclaimer: Please note – This blog is NOT medical advice. This blog is NOT a expert medical opinion on various topics. This blog is purely for information research only and do check the sources where cited. Please DO consult your own doctor to discuss concerns and options, which are relevant and specific to you. The views expressed in this blog are NOT, in any way whatsoever, intended to be a substitute for professional advice. The blog is NOT previewed, commissioned or otherwise endorsed, in any way, by any organisation that the author is associated with. The views expressed in this blog likely represents some of the author’s personal views held at the time of drafting the blog and MAY CHANGE overtime, particularly when new evidence comes to light.